VO2 max measures the maximum amount of oxygen your body can use during intense exercise, usually in mL/kg/min. It is one of the most widely used markers of cardiorespiratory fitness, endurance potential, and long-term health risk.
Below are the most useful VO2 max statistics for benchmarking performance, understanding age-related decline, comparing men and women, and seeing how VO2 max connects to mortality, heart health, training response, and wearable accuracy.
VO2 max statistics
Key VO2 max statistics
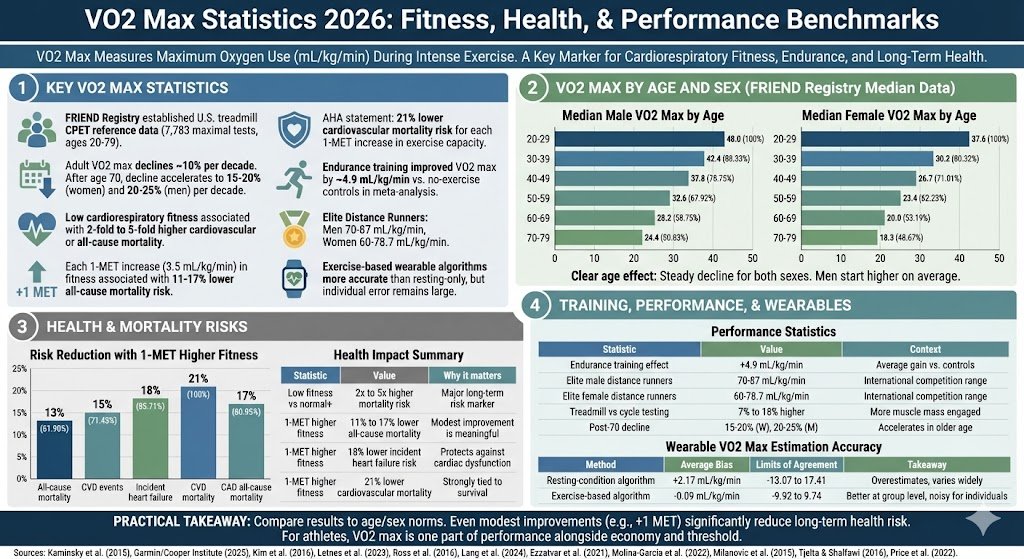
The FRIEND registry established U.S. treadmill CPET reference data using 7,783 maximal exercise tests in adults aged 20 to 79.
In FRIEND, the median male VO2 max falls from 48.0 mL/kg/min at ages 20 to 29 to 24.4 at ages 70 to 79.
In FRIEND, the median female VO2 max falls from 37.6 mL/kg/min at ages 20 to 29 to 18.3 at ages 70 to 79.
Measured adult VO2 max declines by about 10% per decade across adulthood in major reference datasets.
After age 70, the decline in peak oxygen uptake can accelerate to roughly 15% to 20% per decade in women and 20% to 25% per decade in men.
Low cardiorespiratory fitness is associated with 2-fold to 5-fold higher cardiovascular or all-cause mortality in cohort evidence.
Each 1-MET increase in fitness, equal to 3.5 mL/kg/min, is associated with an 11% to 17% lower all-cause mortality risk in meta-analytic evidence.
Each 1-MET increase in fitness is associated with an 18% lower incident heart failure risk in overview-level evidence.
A 2016 AHA statement reported a 21% lower cardiovascular mortality risk for each 1-MET increase in exercise capacity in both men and women.
A meta-analysis found endurance training improved VO2 max by about 4.9 mL/kg/min versus no-exercise controls.
International-level elite distance runners typically report VO2 max values of 70 to 87 mL/kg/min in men and 60 to 78.7 mL/kg/min in women.
In wearable validation studies, exercise-based VO2 max algorithms were much more accurate than resting-only approaches, but individual-level error remained large.
VO2 Max by Age and Sex
Measured treadmill CPET data show a clear age effect for both sexes. Men start higher on average, but both men and women show a steady decline across each decade of adulthood.
VO2 max is not just a performance metric. Large cohort studies and meta-analyses consistently show that cardiorespiratory fitness strongly predicts mortality, cardiovascular events, and chronic disease risk.
Low cardiorespiratory fitness is commonly defined as the lowest quartile or quintile on exercise testing and is linked with 2-fold to 5-fold higher cardiovascular or all-cause mortality.
Each 1-MET increase in cardiorespiratory fitness is associated with an 11% to 17% lower all-cause mortality risk.
Each 1-MET increase is associated with an 18% lower incident heart failure risk.
The AHA reported a 21% lower cardiovascular mortality risk for each 1-MET increase in exercise capacity.
Among patients with coronary artery disease, each 1-MET increase in fitness is associated with a 17% lower all-cause mortality risk.
High versus low fitness was associated with a 69% lower incident heart failure risk in overview-level evidence.
Risk Reduction Associated with a 1-MET Higher Fitness Level
Even modest improvement can be clinically meaningful.
1-MET higher fitness
18% lower incident heart failure risk
Fitness protects against future cardiac dysfunction.
1-MET higher fitness
21% lower cardiovascular mortality
Higher VO2 max is strongly tied to survival.
Training and Performance Statistics
VO2 max is trainable, but the size of the change varies by age, baseline fitness, training history, and exercise mode.
Meta-analytic evidence found endurance training improved VO2 max by about 4.9 mL/kg/min compared with no-exercise controls.
International-level elite male distance runners typically report VO2 max values from 70 to 87 mL/kg/min.
International-level elite female distance runners typically report VO2 max values from 60 to 78.7 mL/kg/min.
Treadmill VO2 max is generally 7% to 18% higher than cycle ergometer VO2 max because more muscle mass is engaged.
The FRIEND dataset showed the measured age-related decline was steeper than older workload-predicted norms from the Cooper Clinic.
Performance statistic
Value
Context
Endurance training effect
+4.9 mL/kg/min
Average gain versus no-exercise controls in meta-analysis.
Elite male distance runners
70 to 87 mL/kg/min
International-level competition range.
Elite female distance runners
60 to 78.7 mL/kg/min
International-level competition range.
Treadmill vs cycle testing
7% to 18% higher on treadmill
Exercise mode changes the final VO2 max number.
Post-70 decline
15% to 20% per decade in women, 20% to 25% in men
The drop often accelerates in older age.
Wearable VO2 Max Statistics
Consumer wearables can estimate VO2 max at scale, but they still do not replace laboratory cardiopulmonary exercise testing when high accuracy is needed for clinical or athletic decision-making.
A 2022 systematic review and meta-analysis included 14 validation studies of consumer wearables.
Wearables using resting-condition inputs significantly overestimated VO2 max by 2.17 mL/kg/min on average.
Resting-based algorithms showed wide limits of agreement from -13.07 to 17.41 mL/kg/min.
Exercise-based algorithms showed much lower average bias at -0.09 mL/kg/min.
Exercise-based algorithms still had wide limits of agreement from -9.92 to 9.74 mL/kg/min.
The meta-analysis concluded that exercise-based methods were useful at the population level, but individual-level error remained too large for many sport or clinical uses.
Wearable estimation method
Average bias
Limits of agreement
Takeaway
Resting-condition algorithm
+2.17 mL/kg/min
-13.07 to 17.41
Tends to overestimate and varies widely.
Exercise-based algorithm
-0.09 mL/kg/min
-9.92 to 9.74
Better at group level, still noisy for individuals.
What These VO2 Max Statistics Mean in Practice
A single VO2 max number only becomes meaningful when it is compared against age- and sex-specific norms and interpreted alongside the testing method used. A treadmill result, a wearable estimate, and a lab-based cycle ergometer result are not directly interchangeable.
For most adults, the biggest practical takeaway is that even modest improvements in cardiorespiratory fitness matter. Because a 1-MET gain equals 3.5 mL/kg/min, moving from 28 to 31.5 or from 35 to 38.5 can represent a meaningful shift in long-term health risk.
For runners, cyclists, and endurance athletes, VO2 max is still important, but it is only one part of performance. Elite results also depend on running economy, lactate threshold, durability, and event-specific efficiency.
Sources
Kaminsky LA, et al. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing: Data From the Fitness Registry and the Importance of Exercise National Database. Mayo Clinic Proceedings, 2015.
Garmin. VO2 Max Standard Ratings. Data reprinted with permission from The Cooper Institute, manual updated August 2025.
Kim CH, et al. The Effect of Aging on Relationships between Lean Body Mass and VO2max in Rowers. 2016.
Letnes JM, Nes BM, Wisløff U. Age-related decline in peak oxygen uptake: Cross-sectional vs. longitudinal findings. A review. 2023.
Ross R, et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice. Circulation, 2016.
Lang JJ, et al. Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses. British Journal of Sports Medicine, 2024.
Ezzatvar Y, et al. Cardiorespiratory fitness measured with cardiopulmonary exercise testing and mortality in patients with cardiovascular disease: A systematic review and meta-analysis. Journal of Sport and Health Science, 2021.
Molina-Garcia P, et al. Validity of Estimating the Maximal Oxygen Consumption by Consumer Wearables: A Systematic Review with Meta-analysis and Expert Statement of the INTERLIVE Network. Sports Medicine, 2022.
Milanovic Z, et al. A Systematic Review and Meta-Analysis of Controlled Trials on Endurance Training and VO2 max. 2015.
Tjelta LIT, Shalfawi SAI. Physiological factors affecting performance in elite distance runners. 2016.
Price S, et al. Differences between Treadmill and Cycle Ergometer Cardiopulmonary Exercise Testing Results in Adults With Overweight and Obesity. 2022.